
RNA Vaccines
Harnessing God’s design to help prevent sickness, but will the new vaccine technology alter our DNA?
Last update: 10 January 2022
Table of Contents
- What are RNA vaccines and how do they work?
- How do Moderna and Pfizer make their RNA vaccines?
- Could an RNA vaccine alter our DNA?
- Pros and cons of the new technology
- How is an RNA vaccine different from older vaccine technologies?
- Other potential concerns
- The Christian’s approach to Operational science

As an organization, Creation Ministries International affirms science. We exist to support the church in proclaiming the truth of the Bible, and thus its Gospel message, mainly by providing real-world answers to the most-asked questions in the vital area of creation/evolution. We are also apolitical and non-denominational (as an organization, not as individuals). We try to confine ourselves to matters as defined broadly by our Statement of Faith, and try not to get involved in needless controversies, both within and outside Christendom, no matter how we, as individuals, might feel about them.
Thus, it might be a surprise to some that we argue against conspiracy theory, that we are generally in favor of vaccination, and that we have a detailed statement that weighs the strengths and weaknesses of the theory of anthropogenic global warming. Each of these areas overlaps our mandate even though we would not consider them essential.
However, we definitely get into areas that are not specifically about creation and evolution when they deal with life and death, such as abortion. Thus, if we can help people understand science, and at the same time steer them away from ideas that could be hurtful or even deadly, we feel this is a good use of our time. As Christians, we have a strong desire to help people. As a science advocacy organization, we feel that we should be using our platform to do just that, when the occasion arises. Since we have taken a clear public stand against evolution, we are clearly willing to go against the tide, no matter how strong its pull. People trust us to present the best information and the best arguments for creation, so we ask that you trust us to do the same here.
Since CMI is a pro-life organization, vaccination is one of the tangential issues we deal with. For a long time, we had no official position on our website, but in recent years we have found ourselves answering more and more questions about them. This has forced us to search for answers to those questions, which then precipitated the publication of a position statement (linked above). Please understand that this only came after much deliberation. It took a lot of time and energy for Dr Jonathan Sarfati to write and multiple CMI scientists were involved in the editing process. In the end, however, the fact that vaccines demonstrably save lives was the deciding factor that made us go public with the information.

There is no question that vaccines have eradicated debilitating and deadly diseases such as smallpox and polio. Improvements and advancements in medical science are a good thing, as they help reverse the effects of the Curse, following Jesus’ example of healing the sick. At the most basic level, it is important to understand that vaccines seek to piggyback on our wonderfully designed immune system by simply introducing something foreign to it. The immune system then reacts by building up antibodies to counteract the foreign substance. The production of antibodies is part of the system, designed by God, that helps our bodies to remember how to fight off infections. Vaccines attempt to train our immune system by giving it ‘target practice’. In the event a person gets exposed to the infectious agent later in life, the immune system will ‘remember’ it and deal with it quickly. From birth, our bodies get exposed to literally thousands of antigens (molecules that can elicit an immune response) daily. Immunizations take up but a small percentage of the total capacity of the immune system.
Due to a massive amount of misunderstanding flying around today, on many different subjects, we feel the need to openly discuss the COVID-19 vaccines that are currently in production. We understand this is a passionate subject for some people. From experience, we find that a significant proportion of antivax information does not come from well-informed sources. This is not to say that all of the information is bad, but misleading arguments are constantly doing the rounds. This greatly concerns us, particularly when considering how common such arguments are in Christian circles. Even people who are generally not influenced by conspiratorial thinking have lots of questions about the new vaccines, us included. But we also know that questions and objections can often be answered by simply stating facts that are properly researched. After everything has been considered, people can then make up their own minds as to how they want to act upon the given information. We shall apply a rigorous approach to the question and try to honestly evaluate what was found.
What are RNA vaccines and how do they work?
There are several COVID-19 vaccines currently on the market. Many more are undergoing trials, but most of these will never see the light of day. Three, however, have made most of the headlines. Not only have they been used (collectively) billions of times, but they use a new technology that has never been used in humans before. All three attempt to get RNA into human cells and then let our cells manufacture a viral protein. This protein can then be ‘seen’ by the immune system, which will then start to produce antibodies to that protein. If everything works as it should, the recipient should now be immune to the disease.
A company called AstraZeneca1 has developed a vaccine that uses a virus to deliver RNA into the cell. This has people worried about the potential for genetic engineering, yet viruses already deliver RNA or DNA to our cells on their own and we don’t call this ‘genetic engineering’. True, the natural activity of viruses is different from the deliberate activity of vaccine scientists, but they are trying to replicate an important part of the cycle of infection while using intelligently designed systems to ward off future infections. Also, the virus in the vaccine is not competent. It cannot start a wave of infection since it only includes one or two protein-coding genes. However, the application of such transfection techniques to humans is potentially more problematic than producing Golden Rice2 and the like, both morally and with regard to the potential (even if unlikely) unforeseeable long-term repercussions. We discuss this further in our main vaccination article, under the subheading Adeno-associated viral (AAV) vector vaccines. This technology was spearheaded by the earlier, successful development of an Ebola vaccine. To date, there are no indicators telling us this strategy is dangerous.
This vaccine had a major hiccup during testing, however, which gives us an excellent illustration about how the vaccine approval system works. The vaccine trials were shut down for a time after one of the volunteer participants became quite ill. It was an open question as to why. They acted properly and halted the trial until they could learn more. Thus, we did not rush these things through at the expense of human health. The matter was cleared up and the vaccine trials started again. Events like this happen in all medical trials. And, as larger and larger numbers of people are included in the later-stage trials, it is expected that some people will get sick for reasons that have nothing to do with the vaccination. People may even die of disease or other natural causes. This is expected to happen when tens of thousands of people are involved. It is then up to the statisticians to determine if the number of sick people has anything to do with the vaccine. Please note that shutting down the trial, temporarily, until things can be investigated, is exactly what is supposed to happen. Thus, even if we were working as fast as possible to produce a working COVID-19 vaccine, regulators were still demanding (as far as anyone can tell) that all safety protocols remained in place.
Moderna3 and Pfizer4 have developed competing vaccines that, while still ‘RNA vaccines’, use a different delivery system than the one AstraZeneca chose. Instead of a living virus, these other vaccines use RNA that has been encapsulated in nanometer-scale droplets of lipids (fat). No, this is not ‘nanotechnology’. This is simply the scale at which cells operate.5 The idea has also been around since at least the late 1990s and one CMI scientist (Philip Bell) worked on a project that was using lipid droplets to deliver a specific drug to the cell around that time. When those lipid droplets bump up against a cell, they will be ingested, along with whatever is contained inside. Thus, in the case of these RNA vaccines the lipids and the RNA are taken in together, in sort of a Trojan horse strategy.
RNA floating freely in the blood is rapidly degraded. It is not turned into protein and so the body would not make antibodies to the virus. This is one reason the RNA must be wrapped in fats. But free RNA inside the cell can also cause an immune response. When detected, the cell will think it is under attack and will raise a signal on the outer cell membrane. When a T cell sees that, it will burst the cell open, preventing any more ‘virus’ from being manufactured. This programmed cell death (technically called ‘apoptosis’) is an important system of regulation in the body. Because of this, the RNA has been engineered to trick the cell into not seeing it as viral RNA. Many of the uracils (one of the four ‘letters’ of RNA) have been replaced with an analogue for uracil during the manufacturing process. The cell can still use the strand to manufacture protein, but it is technically not ‘RNA’. So, if the lipid droplets are absorbed by the cell, and if the modified RNA escapes degradation, only then will the cell begin to manufacture the desired protein.
Some of that protein will eventually make its way to the outer cell membrane. When seen by the immune system cells, they will begin to make antibodies for that protein. But the body also thinks these cells are infected, so a macrophage (a type of white blood cell) will come along and gobble the cell up. Yes, any cell that ingests the viral RNA strand will die. But considering that this happens in your body constantly, and considering that you have trillions of cells in your body, sacrificing a few in order to produce a protective antibody is inconsequential.
However, this will still be introducing foreign RNA to the human body. Nobody can say that there is a zero percent probability that the RNA in the transfected cells cannot jump to other somatic cells, in which case this might lead to more serious autoimmune complications. On the other hand, we cannot say with 100% confidence that this will not happen naturally when a person is exposed to any virus in the wild. And, if you think about it, the cycle of introducing RNA into a cell, getting the cell to express foreign proteins, and watching the body’s response to those proteins is actually more natural than older vaccine technologies. Proteins are not being injected into the bloodstream. Instead, the body is more closely following what happens during a normal viral infection, which by necessity happens inside human cells.
How do Moderna and Pfizer make their RNA vaccines?
No matter what you think of the safety and efficacy of the mRNA vaccines (our main article on vaccination makes the case that they are both safe and effective, by the way), the process of manufacturing the new vaccines is still ingenious:
- Scientists start with a DNA code typed into a computer and use a DNA synthesizer (essentially a ‘DNA printer’) to manufacture it. They then insert the DNA segment into a circular piece of DNA called a plasmid and trick E. coli bacteria into absorbing it. As the bacteria grow, they make many copies of it.
- This DNA is harvested and then turned into RNA in a test tube using bacterial enzymes.
- Using a series of chemical reactions, the RNA is wrapped in lipid envelopes, while still in a test tube, and stored at –80°C to prevent the breakdown of the RNA.
How do RNA vaccines work?
- When injected into muscle tissue, the cells ingest the tiny fat droplets, thus bringing in the RNA as well. Protein synthesis begins, but if the cell detects foreign RNA, it commits suicide (apoptosis), through the action of T cells.
- If the RNA escapes cellular detection, it will be translated into protein.
- Some of the protein should make its way to the outer cell membrane, where it will trigger an immune response, the production of antibodies, and the death of the cell via ingestion by a macrophage (white blood cell).
- At least one of these RNA vaccines includes a section of DNA from an alphavirus that codes for self-replication. This “self-amplifying RNA” (saRNA) requires a smaller dose because the cell will make more copies of the RNA after it arrives, but the cell will still be slated for destruction as soon as it starts producing foreign proteins.
There were about 60,000 people in each of the stage-3 vaccine trials, with about half getting a placebo. Thus, on the order of 50,000 people received an RNA vaccine during testing. No problems (statistically) were reported. We say ‘statistically’ because in any given cohort of that size some people are going to die, get cancer, or become otherwise ill over the course of several months.
Could an RNA vaccine alter our DNA?
Being that this is a brand-new technology, people have serious concerns about safety. On top of the list are questions about genetic engineering. Is it possible that the vaccine could change our DNA? Repeating some of the information above, here is a list of reasons why the probability is vanishingly small:
- Viruses already inject DNA and RNA into our cells. With rare exceptions, this material does not make it into our genome. The HIV virus is notorious for making copies of itself that then get incorporated into our DNA, but they have specific mechanisms and genetic sequences for doing so. The RNA in the new vaccines has none of those features. Even though the wild version of the virus used in the AstraZeneca vaccine can also do this, it is not known to cause any diseases. Even so, the RNA contains but one or two protein-coding genes. This is not enough information to do anything in the cell.
- Our cells produce massive amounts of RNA already. This goes from the nucleus to the cytoplasm, where it is translated into protein. There is no evidence for widespread re-incorporation of RNA into the human genome. In fact, the whole system would collapse if there were not safeguards preventing this from happening.
- The amount of RNA being used is minimal.
- Any cell that takes up the foreign protein gene will be killed by the immune system. At least, this is what is supposed to happen and indeed is what does happen in nearly all cases. A person whose body fails to respond in this way is at a high risk of death from any infection, and the RNA vaccine is not an infectious agent. The immune system is exceptionally complex, and we cannot say that every single person will respond in the same way. But if this is a concern, it should be a concern for all viral infections as well.
- The arm muscles are far from the gonads. So even if some cells incorporate the RNA (in the form of DNA) into their genomes, it will be difficult to pass this to the next generation. Again, nobody can say it is impossible, but there is little reason for considering it to be probable. Then again, we have sometimes been surprised by biology.
Considering all these points together, as a scientist with a strong background in genetics, I believe the risk of the ‘genetic engineering’ of people is extremely small—thus, it was not sufficient to warrant halting the vaccine trials and it is not sufficient to warrant halting the widespread use of the vaccines today. We can always be surprised, but everything we do know tells us that the new technology should be safe. And that is an important consideration. Even when acting out of an abundance of caution, we have to make final decisions based on positive knowledge, not the fear of potential unknowns. This is something that applies to daily life. If we cannot make decisions based on what we know, we would be paralyzed with fear and unable to do anything. We could not eat for fear of food poisoning. We could not drive for fear of drunk drivers. Thus, the goal is to study this new idea until every significant concern has been addressed. After that we can proceed, cautiously, while re-assessing every serious concern at each step. This, indeed, is what we did.
Pros and cons of the new technology
The incorporation of any new technology comes with tradeoffs. This is an inescapable fact of human existence. The new vaccines are no different.
Pros:
- No fetal cells are required! Happily, no fetal cells are used for the steps outlined above. However, for testing purposes only, the Moderna vaccine used the HEK293 cell line, which was derived from either an elective abortion or a spontaneous miscarriage in the Netherlands in 1973. HEK293 has become a workhorse in laboratories worldwide. Sub-strains have even been created by genetically tailoring the cells for specific purposes. We cannot change history, but please see CMI’s official position on the situation. That article has been updated with information regarding the new types of vaccines, the current pandemic, and the alarmist arguments about using ‘baby parts’ in vaccines. We also cannot guarantee that these cells were not used somewhere in the supply chain or that some significant advance that allowed the eventual development of the vaccine was not made using these cells. On the other hand, this is an amazing step in the right direction. The use of fetal cells was minimized, and NO BABY PARTS are in the vaccine itself.
- We can now go from a DNA sequence to a viable vaccine candidate in a matter of days. Most of the vaccine development time, therefore, will be in the testing stages. This is amazing progress. It should have clear economic impacts as well.
- The use of adjuvants is made obsolete. An adjuvant is something designed to stimulate the immune system.6 Essentially, it wakes the immune system up so that it starts looking for foreign antigens. Currently, aluminum salts are the chosen adjuvant in many vaccines (at physiologically irrelevant levels, btw). Another common adjuvant is squalene, which can be obtained from the livers of certain sharks. The RNA vaccines require no adjuvants at all, although the lipid coating can be tailored for such purposes, if required. Freely circulating RNA also acts as an adjuvant, making the immune system believe there is an infection taking place.
- The need for preservatives (e.g. mercury) is eliminated. Since RNA is so fragile (it breaks down in water 100 times faster than DNA), it must be stored in very cold temperatures anyway. Thus, adding extra preservatives is made irrelevant.
Cons:
- This is an unknown technology. We will not know what will really happen until we release it into the public arena. However, this is always true with everything we do. Using common sense and past experience, most potential problems can be avoided. [Note: this was written before the vaccines were fully deployed. They have now been in use for nearly two years and billions of doses have been given. We know a lot more now than we did then, and for the most part (rare complications have been noted for one vaccine in particular), the vaccines have not raised red flags.]
- We do not know that there will be zero long-term problems. There are many examples of pharmaceuticals that passed through every stage of testing, and only on being approved for use were terrible side-effects manifested. Yet, this could be said of any new product in any area of society. There is a difference between a toaster and a vaccine, however, which is why these companies spent so many millions of dollars in safety testing.
- The temperature requirement means it will be difficult to distribute in many places in the world. The Moderna vaccine, however, is reported to be stable at normal freezer temperatures and lasts for up to a month in a refrigerator.
- There is no way to know if the vaccines have not decomposed. Being that they are so labile (because RNA is such a sensitive molecule), this is a serious concern. Yet, despite a couple of mishaps, this has not been a problem.
- Note that the vaccine itself will likely produce a slight fever, mild chills, and a light rash near the injection site in some people. It is possible that a patient might feel bad for a day or two after getting the vaccine. However, this is evidence of a robust immune response. The body is mustering its resources to attack a perceived invader and those symptoms are the result. Yet, the symptoms are not COVID-19 itself, for one simply cannot get the disease from the immunization. There will be no virus present. [Note: people have reported a range of responses to the vaccines, from not even noticing to feeling sick for weeks, but the normal response is what I initially wrote.]
How is an RNA vaccine different from older vaccine technologies?
Most vaccines utilise killed or weakened organisms. Some of the more recently developed ones use genetically modified yeast or E. coli to grow up a batch of antigens (molecules that can elicit an immune response) that can then be incorporated into a vaccine. The strategy was to inject proteins or sugar chains into a person that could then trigger the production of protective antibodies.
When vaccines were first developed, we did not even know what viruses were. All we knew was that we could take pus from a cowpox scab and inject it into a person’s arm. Yet, this would then protect a person from smallpox. Edward Jenner was the first to do this, in 1798, ushering in the era of vaccination. Louis Pasteur, noted by us for his outspoken belief in creation, also developed attenuated (that is, live, but non-viable/disabled bacteria) vaccines for anthrax and cholera. Other early vaccines (e.g. tetanus and diphtheria) used bacterial toxins denatured by formaldehyde, making them harmless but still able to produce a strong immune response. These diseases were worldwide scourges, causing untold amounts of suffering and death annually. The early vaccines were used to greatly reduce the disease burden on society, but they would not pass modern safety standards.

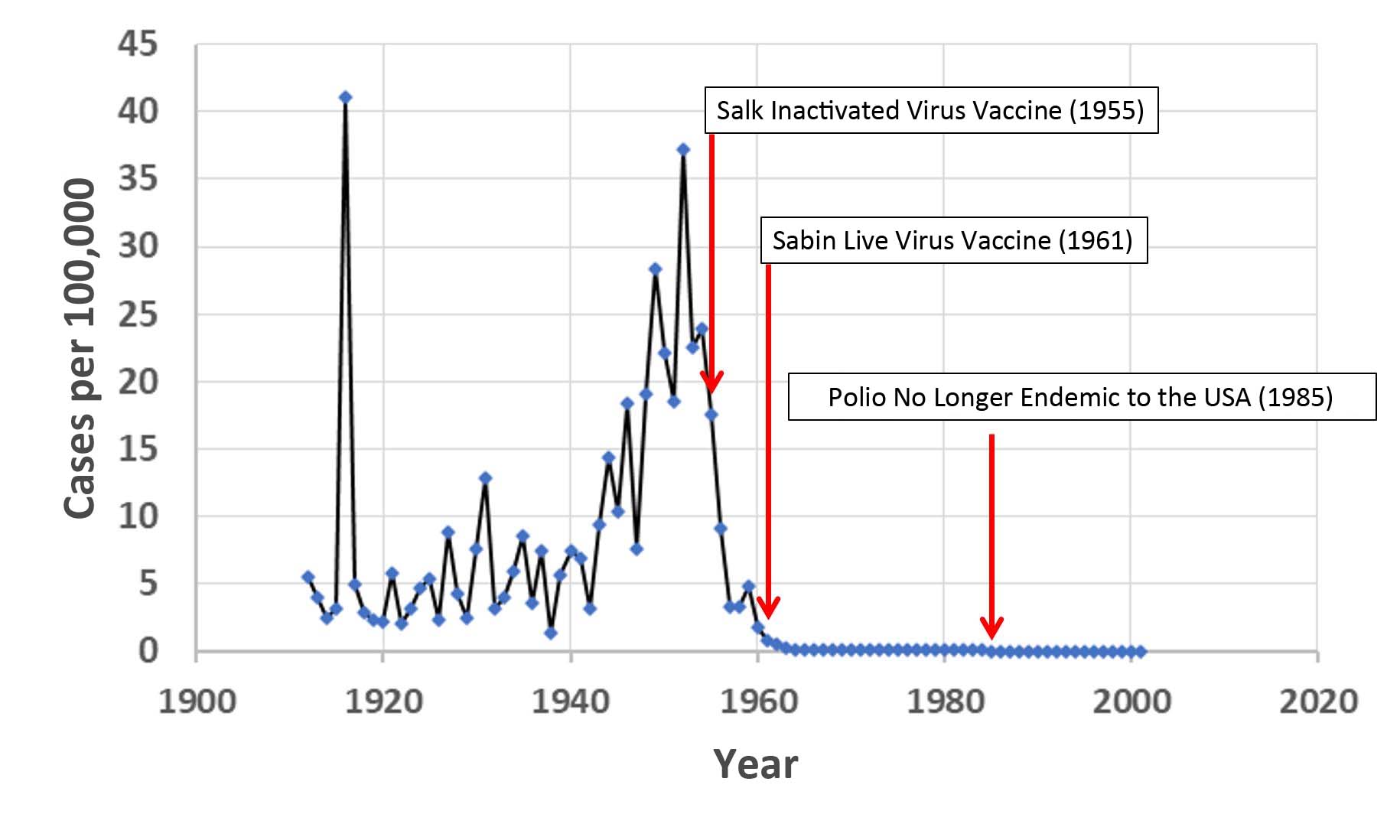
In the 1950s, two competing polio vaccines were developed. The Salk vaccine used dead viruses. It was widely used, and highly effective. But it fell into disfavor after two manufacturers failed to properly inactivate the virus, causing multiple cases of polio and even a few patient deaths. The Sabin vaccine that replaced it used live attenuated viruses. At least one version of the polio vaccine was injected into a series of mouse and rat brains. At the end of this serial process, the (now attenuated) virus was no longer able to infect human nerve cells. Today, polio is nearly eradicated worldwide, but we are seeing problems with the polio vaccine. In some places it is popping up after people receive the live attenuated (weakened) virus in the vaccine. Health authorities are well aware of the problem and are doing everything they can to work around it. Using weakened viruses is not always a perfect solution and so we should be looking for new ideas, perhaps like an RNA vaccine.
Historically, the most commonly used influenza vaccines were grown in chicken eggs. This was true for over 70 years. Both the heat killed (inactivated) and live (attenuated) versions of the vaccines were made from egg-cultured viruses. However, as of 2020, most influenza vaccines have been grown in mammalian cell culture. This is either VERO (African green monkey) or mouse cells, because using human cells (like HEK293) would produce a virus that could easily infect people. Recombinant flu vaccines also exist. Here, a microorganism (yeast or E. coli) is engineered to express a viral protein, which is then harvested and incorporated into a vaccine.7
All of these vaccine technologies have disadvantages compared to the new RNA vaccines.
Other potential concerns
- Operation Warp Speed (as designated by the US government at the time) raised questions about risks to human health. Did we rush things? Did we cut too many corners? Did we move too fast? These are honest questions that need to be asked. Yet, much of the time historically spent in vaccine development involved massive amounts of paperwork, long periods for governmental review, and things like that. This is not a discussion on free market capitalism, but an advanced society should be able to act efficiently. Any governmental policy that helps to unleash more creative potential should be a net positive. Of course, cutting corners and overall safety are always a concern, but Operation Warp Speed was designed to reduce red tape while not reducing safety, and it effectively attained those goals. Moderna is a new company and accepted money from the US government to assist in vaccine development. Pfizer used no government funds to develop the vaccine but it did accept a large amount to help build the industrial infrastructure required to quickly produce up to a billion doses.
- Runaway super pandemic: Some people are worried that the vaccine might actually cause a worse disease than it is designed to prevent. Yet, no viral structural proteins are encoded in the RNA. They are targeting one protein only (the spike protein), and it has been modified (in other words, it is not the naturally occurring version). There is no way to make a complete virus from that one gene, and any virus that took up the modified gene would probably be defective anyway.
- Evolution of a newer, more deadly virus: The virus is not evolving; it is mutating. We must understand the difference. Also, SARS-CoV-2 is not an influenza virus. Flu viruses tend to change a lot from year to year. Reassortment among viral strains creates new viruses that are new to our immune systems (e.g. H1N1, H3N2, and H5N7). Thus, we need a completely different flu vaccine every year. Unlike the influenza genome, which is broken up into multiple RNA strands, the genome of SARS-CoV-2 is a single, unbroken piece of RNA. Even though recombination among different coronaviruses can occur when an animal is infected with two different viruses at the same time, influenza viruses reassort much more frequently. The threat of a new, more deadly virus arising via recombination among coronavirus subtypes is less than the rise of new influenza serotypes. Also, the history of coronaviruses shows us that they burn hot when they first enter the human population, but then attenuate over a few years. For example, one of the coronaviruses that causes the common cold, OC43, shares a high sequence similarity to a coronavirus that affects cows. Molecular clock estimates place the split between these two viruses about 130 years ago, or about 1890.8 This is the same timeframe of the “Russian Flu” pandemic of 1889–1890 that killed at least one million people. Queen Victoria’s grandson, Prince Albert Victor, died of the Russian ‘flu’, but the virus is almost irrelevant today as far as human health is concerned. In the end, we want the virus to mutate because mutation accumulation is bad for the virus. Yet, we also want people to be aware that it will take a few years before the bug attenuates to the point where it is nothing more than a common cold. Also, while this is occurring, it is possible for a new serotype that our immune system does not recognize to appear (the Omicron strain came close). It is also possible, in fact likely, that a version of the virus that spreads faster will emerge (e.g., Omicron). At present, the latest viral strains present the same image to our immune systems as the older ones, although authorities are keeping a careful watch on several strains that have emerged recently. There is, currently, no indication that the vaccines will not work in the future, but vaccine companies are ready to start producing new vaccines, if necessary. In the end, mutation is generally a bad thing for a virus, but attenuation takes time and mutations can cause mischief as we wait.
- Eschatology: Except where it intersects with the book of Genesis, CMI does not maintain an official position on end times theology. However, many people still write in with questions about end times, the pandemic, and the resulting rush to produce a vaccine. We answer as best we can, based upon the facts before us. But this is not something we are going to answer directly because it is simply outside our mandate.
- There are other potential concerns that have nothing to do with the new technology. People are still asking about them, and so the questions tend to get jumbled in our minds. We can quickly dismiss conspiracy claims that this involves Bill Gates, ‘aerogels’, ‘biochips’, or tattooing people with a vaccine. None of this applies to the current vaccines. There is some scuttlebutt circulating about ‘vaccine tattoos’, but even if implemented, public acceptance of such a thing is going to be very, very low. The thought is that one could generate a code in the form of invisible titanium dioxide dots that coat an array of microneedles. When the needle array is applied to the skin, the dots would remain behind and could then be detected for several years afterward. Most middle-aged adults who had a smallpox vaccination as a child still have a small, raised area on their skin. So what? Back then, nobody seemed to be worried that this was some marker that was going to hasten the end of the world. Regarding the ‘biochips’, these are the PIT (passive integrated transponder) tags that are used routinely in animal husbandry and for identifying pets. I even incorporated them into the glue that was holding many of my coral specimens in place while performing experiments in grad school. I was instantly able to tell the colonies apart by simply waving a wand over them and reading the results on a screen. Yes, these are small, and yes, they can be inserted under the skin. But there are physical limits to transmitter technology. They cannot get much smaller than they already are and the tags are passive. They simply cannot transmit any signal on their own. The detectors also do not work when more than a few centimeters away. Either way, I have no plans on getting tagged or tattooed, and I have no reason to fear having this done to me against my will. We have already dealt with questions about the genetic engineering of humans and the use of fetal cell lines.
The Christian’s approach to Operational science
Putting all claims of conspiracy and subterfuge aside, the development of vaccines should be a simple matter of applying operational science to a bad situation. Please read up on why operational science has little to do with the creation vs. evolution debate. We are not arguing over the boiling point of water or the force of gravity. These are matters of operational science that stand on their own merits. Historical science, on the other hand, is intrinsic to the debate. We are definitely arguing over matters that occurred in the past and the degree to which operational science can, or cannot, inform us about past events. We should not mistake these two forms of science. Even if the evolutionary community has consistently done so, this does not mean we should. On the other hand, we should also not fall off the other side of the horse. Just because historical science has been abused, this does not mean we should reject operational science, as the flat-earthers and geocentrists do. If we are to draw a line in the sand, it should be between historical and operational science, neither conflating the two nor jettisoning operational science. This has always been CMI’s position. Our statements to this effect go back decades. We are not anti-science, nor are we being contrarians just for the sake of it.
In the end, we have to understand that foreign DNA and RNA gets into our cells all the time. This is exactly how viral infections work. Yet our bodies almost always fight them off. We are actually bombarded with viruses on a daily basis. It is clear, therefore, that we have a robust way of dealing with them. The new RNA vaccine technology is simply harnessing something that already exists, a system designed by God. In some sense, this is little different from taking vitamins and medicines, since these are designed to work with God’s created biology. The fallen world is imperfect, but we have to do the best we can with what we are given. Harnessing God’s amazing design to relieve human suffering is a good place to start.
References and notes
- See www.astrazeneca.com/covid-19.html. Return to text.
- Golden Rice is a genetically engineered version of Oryza sativa (rice) that produces beta carotene in the endosperm (the starchy part humans like to eat). Rice already produces beta carotene, but only in the leaves. Scientists took a gene from daffodils and another from a bacterium (which was later shown to be unnecessary) and inserted them into the rice genome next to a promoter that controls genes that are only expressed in the endosperm. The result is a strain of rice that produces copious amounts of a substance that is deficient in the diets of a significant portion of the world population. Whether or not this amount of beta carotene will have any positive effect on human nutrition has yet to be determined. Return to text.
- See www.modernatx.com/modernas-work-potential-vaccine-against-covid-19. Return to text.
- See www.pfizer.co.uk/behind-science-what-mrna-vaccine. Return to text.
- 1 nanometer (nm) = 10-9 metre. Thus, 1 mm = 1 million nm! Return to text.
- cdc.gov/vaccinesafety/concerns/adjuvants.html. Return to text.
- cdc.gov/flu/prevent/how-fluvaccine-made.htm. Return to text.
- Vijgen, L. et al. Complete genomic sequence of human coronavirus OC43: molecular clock analysis suggests a relatively recent zoonotic coronavirus transmission event. J Virology 79(3):1595–1604. Return to text.



Readers’ comments
Comments are automatically closed 14 days after publication.